Individuals with presbycusis initially experience hearing loss at higher frequencies, which significantly hampers communication, particularly in environments with background noise or echo. As the condition advances and hearing loss extends to the 2–4 kHz frequency range, the ability to accurately perceive words, consonants, and even vowels becomes more difficult, leading to increased thresholds for auditory recognition [3]. ARHL can lead to emotional challenges such as feelings of loneliness, social withdrawal, depression, and heightened anxiety [4-6]. ARHL can vary in severity, often affecting both ears symmetrically, and may lead to challenges in communication, social interaction, and overall quality of life [7]. While the progression of this condition is generally permanent, early detection and appropriate interventions, such as hearing aids or assistive devices, can help manage the impact on daily life [8]. In 2020, the global economic losses due to untreated hearing loss amounted to nearly 1 trillion international dollars [9]. Effective and cost-efficient approaches for the identification and rehabilitation of hearing loss are already benefiting millions of individuals across various age groups. By combining these interventions with public health strategies, it is possible to extend their reach to all those in need [10]. The global burden of hearing loss, measured in YLDs, has increased significantly over the past decades, with a linear increase of 18.7% in the past ten years [11]. Most existing studies focus on the prevalence of hearing loss within specific countries. There is limited research addressing the South asia region. The region faces unique challenges due to its large population, diverse socio-economic conditions, and varying levels of healthcare infrastructure. ARHL in South Asia is not only a medical concern but also a socio-economic one, affecting individuals' quality of life and productivity [12, 13]. In South Asia, this issue represents a formidable challenge, compounded by a lack of trained healthcare professionals, limited human resources, and inadequate diagnostic facilities, which together hinder effective management and intervention [14]. This study aim to analyze the prevalence and disability burden of ARHL in South Asia from 1990 to 2021, using data from the Global Burden of Disease Study 2021. It examines temporal trends in ARHL prevalence and YLD, while providing projections for 2031 to guide future public health strategies to address this public health challenge.
Methods
Data sources
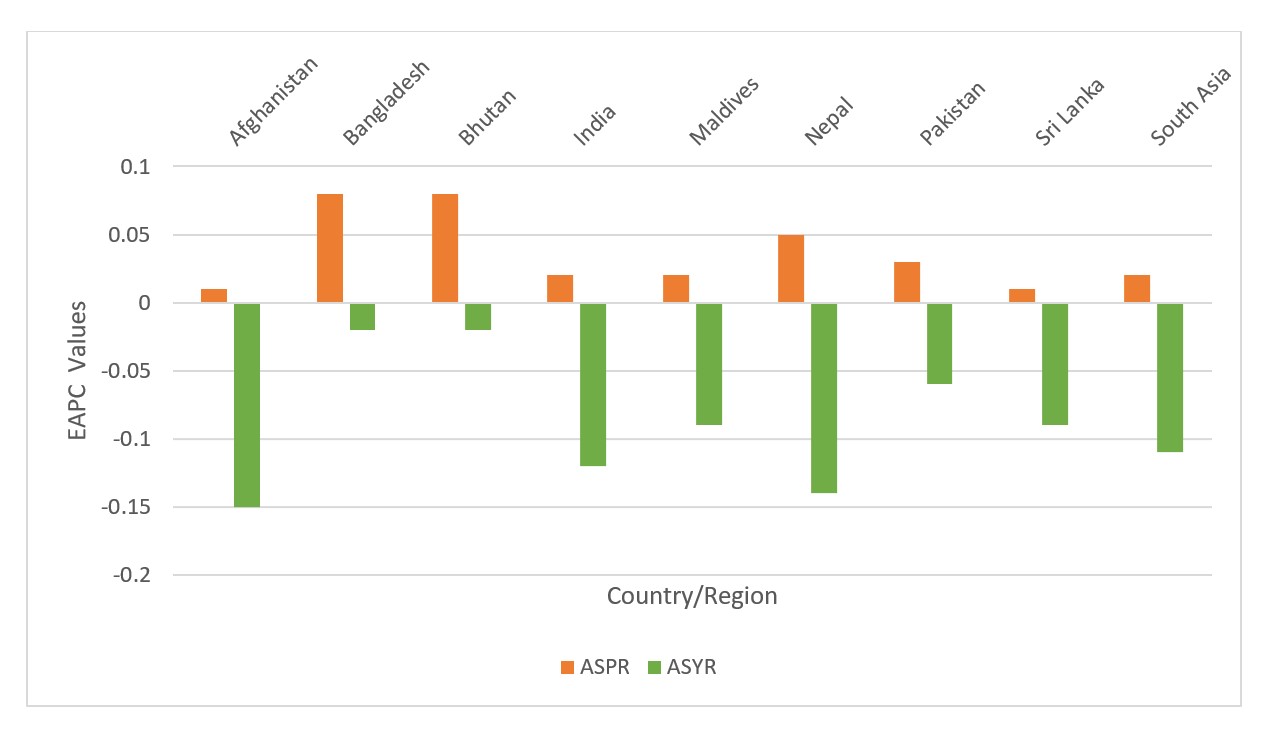
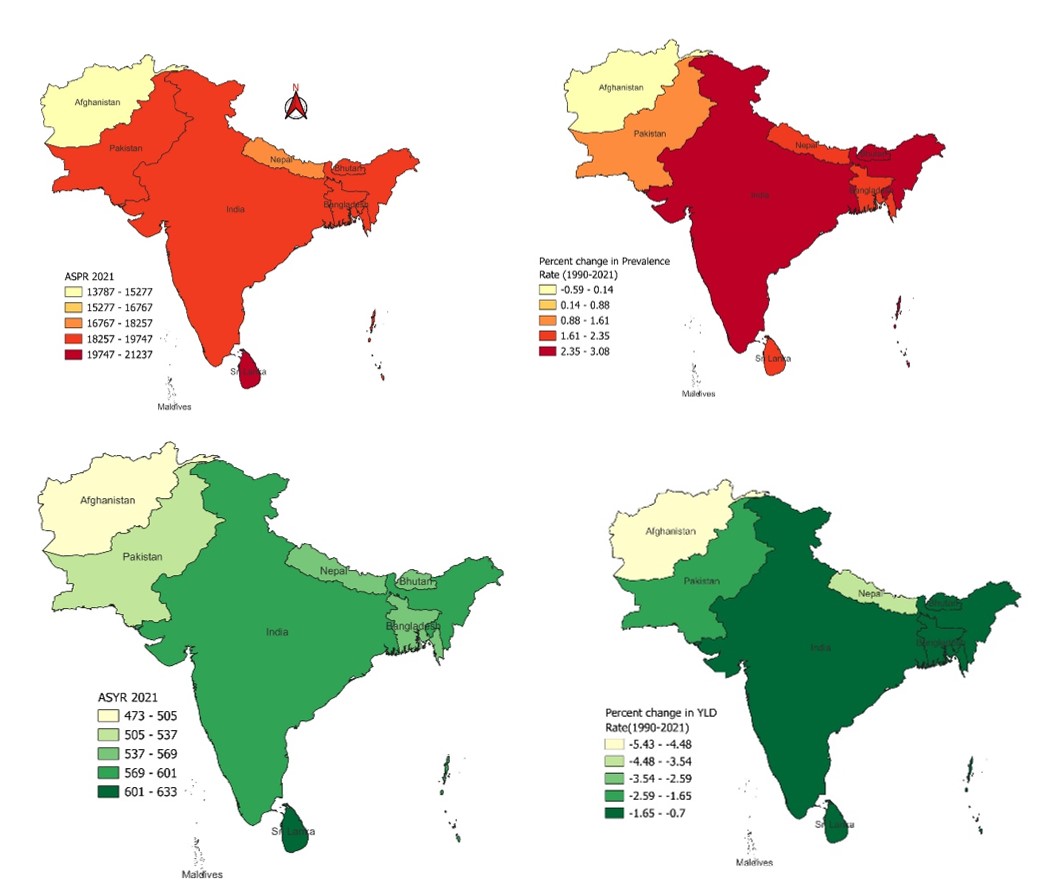
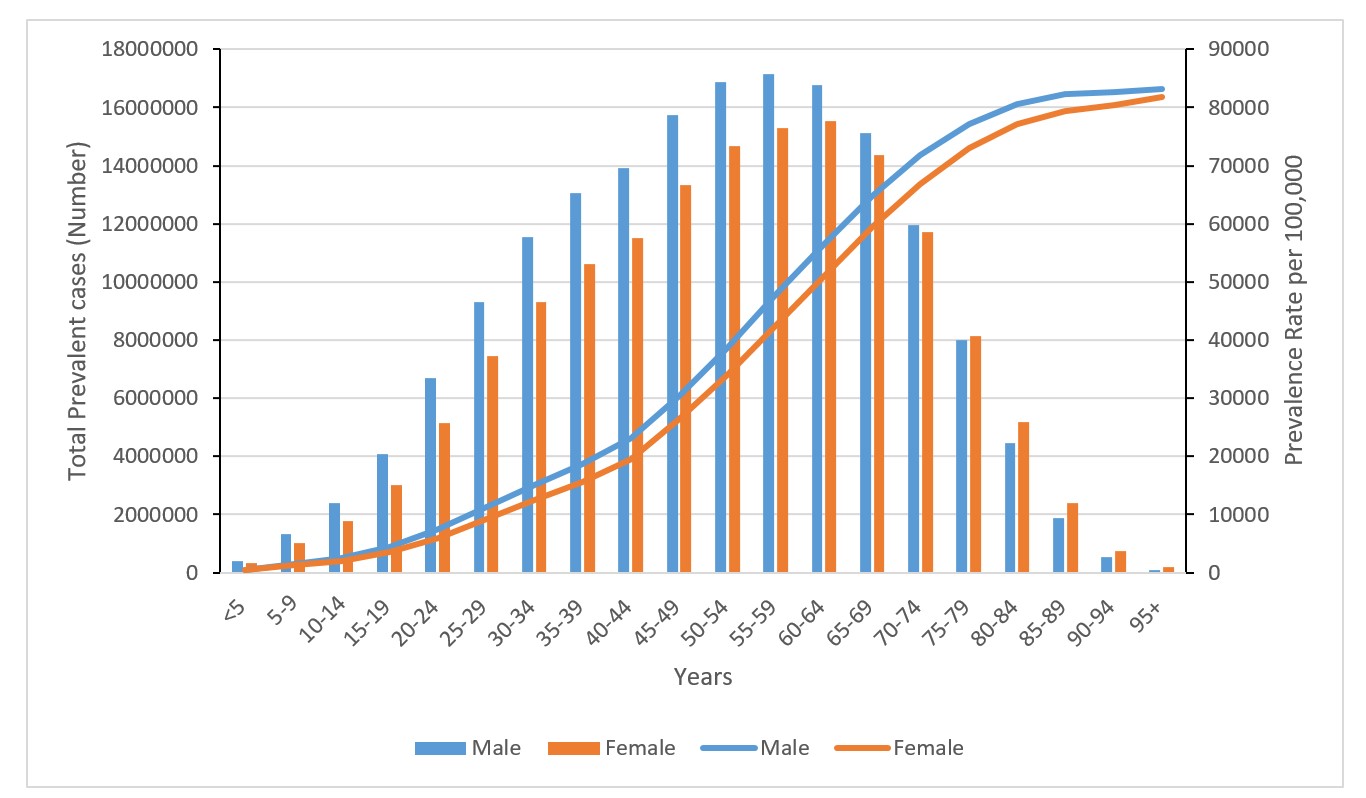
The GBD 2021 study provides an extensive assessment of health loss associated with 369 diseases, injuries, and impairments, and 88 risk factors across 204 countries and territories, using latest epidemiological data and refined standardized methods. All results are available via the GBD Compare website [15], and all input data is identified via the Global Health Data Exchange website [16]. This study utilizes data from the GBD 2021 to assess the prevalence and disability burden (YLDs) of age related hearing loss in South Asia, covering the years 1990 to 2021. The analysis incorporates ASPR and age-standardized YLD rates (ASYR) and its numbers across eight countries: Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka. The data was disaggregated by age and sex to examine differences in the impact of hearing loss across various demographic groups. Prevalence and YLD numbers were analyzed across different age categories, revealing trends in ARHL and its associated disability burden over time.
Statistical analysis
Joinpoint regression analysis
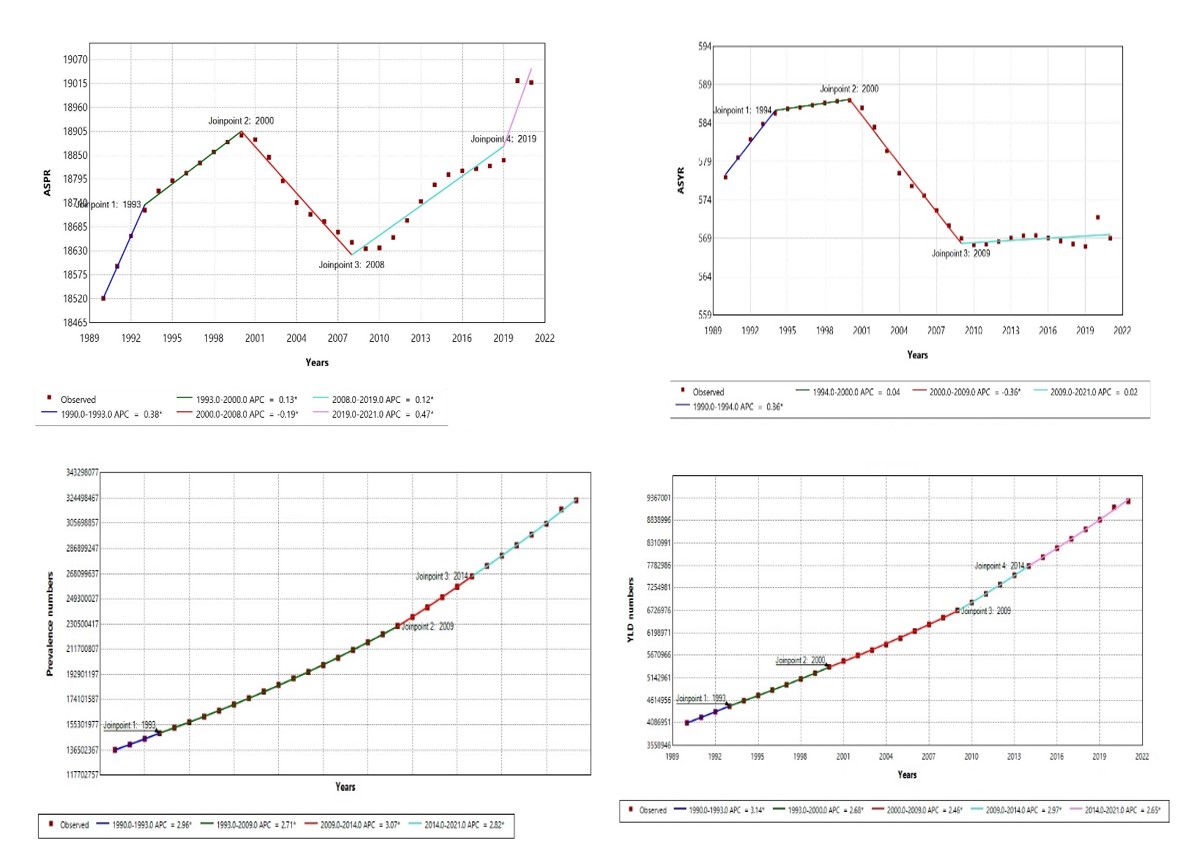
Joinpoint regression analysis was used to identify significant changes or "joinpoints" in the trends of age-standardized prevalence and YLD rates for ARHL in South Asia. The analysis was conducted to detect periods of accelerated or decelerated trends in the rates from 1990 to 2021. This method allowed for the segmentation of the trend into distinct periods, each with its own slope, thereby providing insights into the temporal dynamics of ARHL prevalence and disability burden. The annual percentage change (APC) in each segment was calculated with 95% confidence intervals, helping to determine the significance and direction of trends over different time intervals.
ARIMA forecasting
To forecast the age-standardized prevalence and YLD rates of ARHL in South Asia from 2022 to 2031, we applied the ARIMA model. This time series forecasting method was chosen for its ability to capture temporal dependencies and underlying trends in the historical data. Initially, differencing