Introduction
South Asia accounts for a substantial portion of global Road traffic injuries (RTIs), with a road traffic death rate of more than 5 per 100,000 population [1]. RTIs are a leading cause of death and disability, particularly among young males and children, with two-wheelers being major contributors to accidents [2]. The economic impact of RTIs is significant, costing billions of US dollars and affecting the Gross Domestic Product (GDP) by 0.3 to 7.5 percent in the region [3].
RTIs not only cause physical harm but also impose a considerable economic burden, which includes both direct and indirect costs. Direct costs encompass property damage, medical treatment, and rehabilitation, while indirect costs involve productivity losses, disability, legal expenses, and insurance claims. Globally, road injuries are projected to cost the world economy nearly $2 trillion between 2015 and 2030, equivalent to an annual tax of 0.12% on global GDP [4]. Developing countries experience higher fatality rates from RTIs compared to developed countries. These countries account for 90% of global road traffic deaths, despite having only about 50% of the world's motor vehicles[5]. In high-income nations, RTIs account for a smaller share of GDP losses [5].
Given the significant challenges posed by RTIs in South Asia, it is essential to assess and quantify their economic burden to inform policy and prioritize public interventions. This study aims to quantify the economic burden of RTIs in South Asia using the Human Capital Approach (HCA). By quantifying the burden, the study provides valuable insights into the economic burden of RTIs, which can guide policymakers in implementing targeted strategies to reduce fatalities, improve infrastructure, and strengthen healthcare systems. Additionally, it highlights the broader implications for economic growth, emphasizing the urgent need for a comprehensive road safety approach in South Asia.
Methods
Data source
Data on the estimated number of deaths from RTIs and life expectancy for both sexes in eight South Asian countries were sourced from the 2021 Global Burden of Disease (GBD) study [6]. The GBD study utilizes an ensemble method to estimate causes of death, incorporating various covariates across different geographic levels, as detailed in previous publications [6, 7]. Covariates included in the RTIs model are described elsewhere [8]. Additionally, data on Government Health Expenditure per capita and GDP per capita at current prices were obtained from the WHO-GHED [9]. All the economic data is taken at current US dollar prices.
Analytical Framework
The economic burden of RTIs was assessed using the HCA, which adopts a macroeconomic perspective to measure the total loss to a country resulting from disease burden [10]. HCA evaluates the economic productivity linked to an individual’s skills or educational training and estimates productivity losses for years of life lost due to premature mortality[10, 11]. This approach has been widely used to estimate the economic burden of various diseases, including non-communicable diseases, injuries, and neglected tropical diseases in different countries [12, 13]. Among the many applications, the HCA has been used to estimate the burden of suicide deaths in India and Africa, and in Canada, it has also been employed to assess the economic impact of implementing prevention strategies for RTIs [10,13]. There are several methods for applying HCA, each with distinct assumptions and nuances that influence the estimates of economic burden.
Economic Analysis
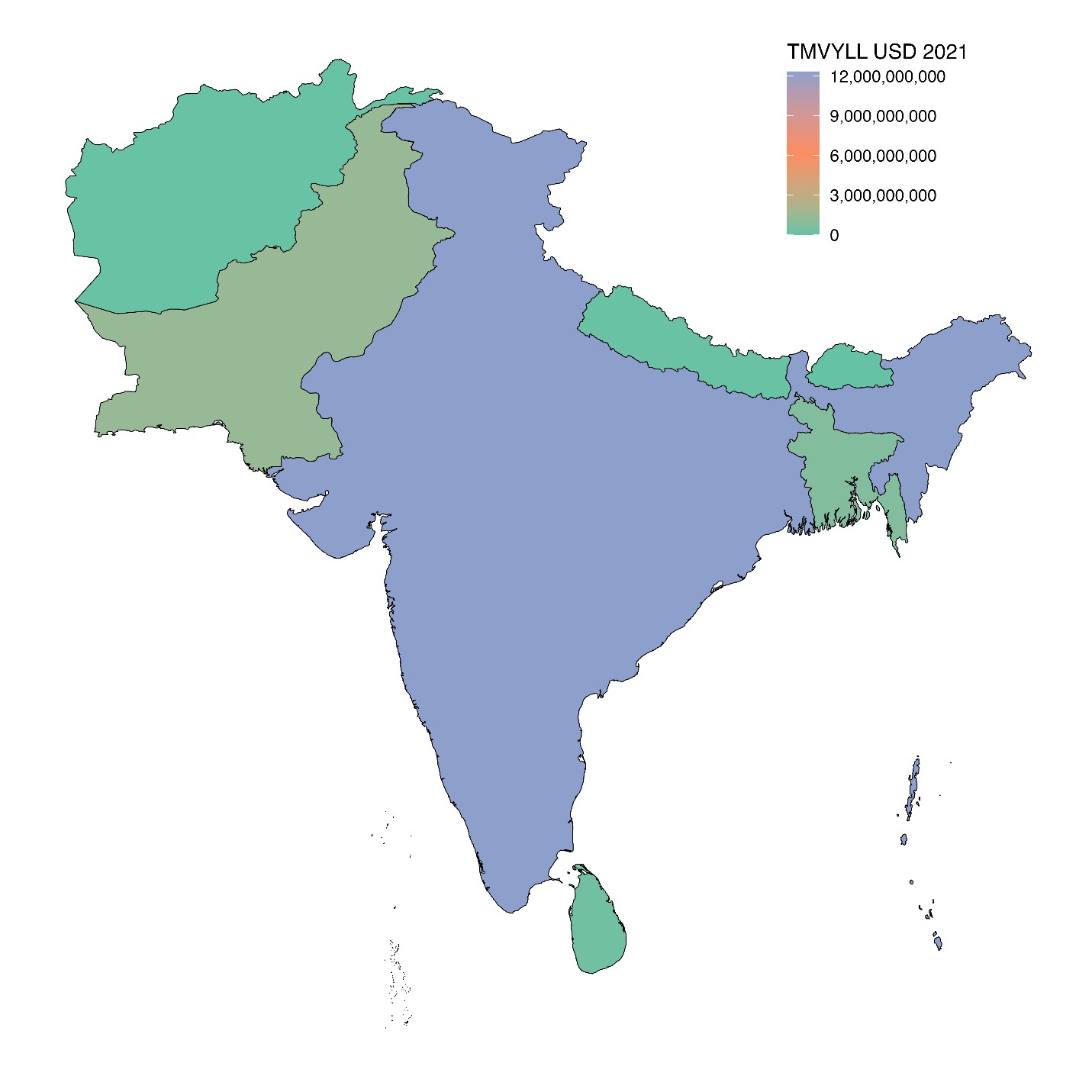
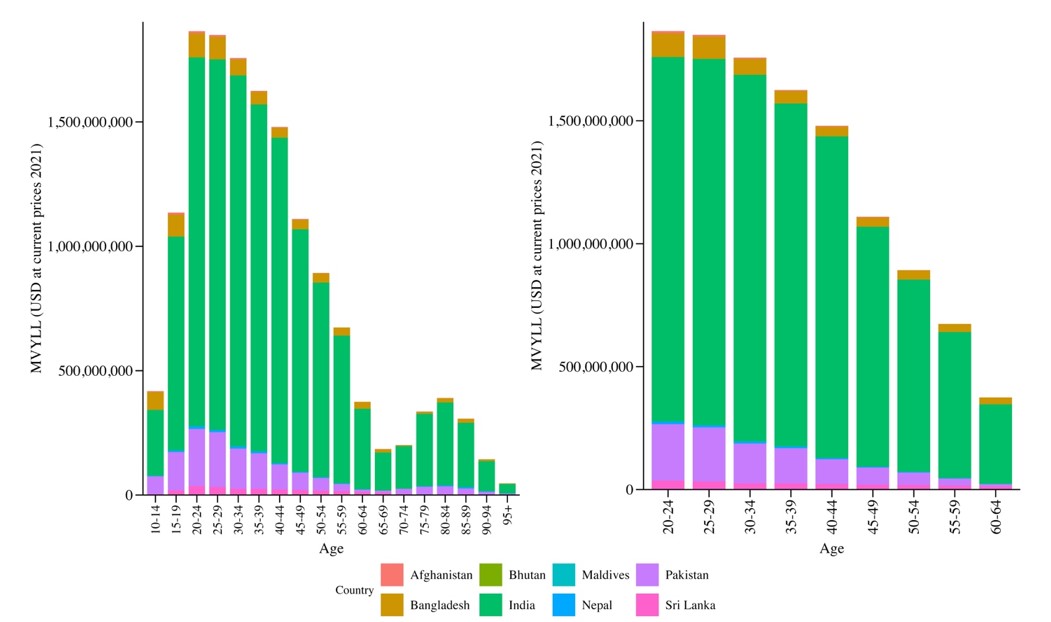
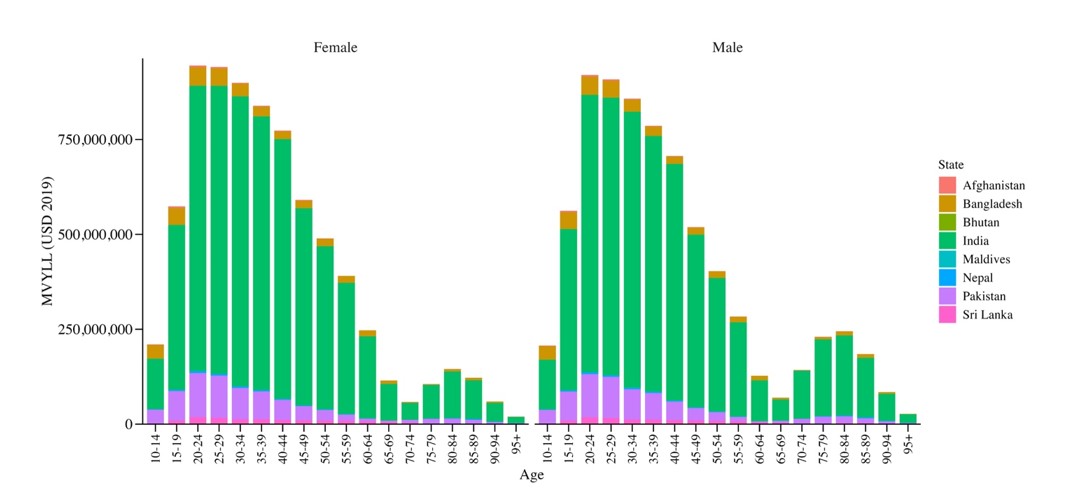
We employed the HCA to calculate the total monetary value of years of life lost (TMVYLL) across 8 countries in 2021. The calculations were performed in line with the methodologies outlined by Nigam et al. [10] and Kirigia and colleagues [13]. We calculated the Monetary Value of Years of Life Lost (MVYLL) for each state (m), each sex (s), and each age group (j) using the formula provided in Equation (1). MVYLL was calculated as the product of the non-health GDP per capita and the number of RTIs deaths, adjusted for discount rates.